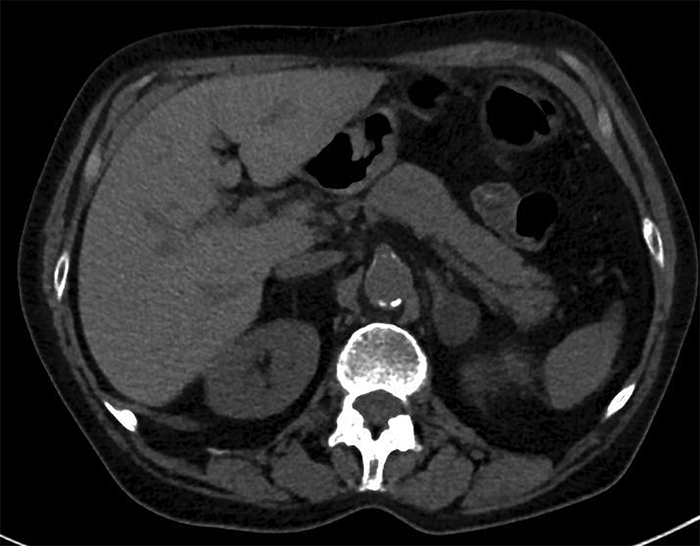
Adrenal masses are often discovered incidentally and are then termed adrenal incidentalomas (AIs). They are often discovered after an imaging procedure is performed that is unrelated to the adrenal gland. Usually, the patient has no signs of hormonal excess or obvious underlying malignancy. Incidence has been increasing proportionally to the use of radiographic imaging. Less commonly, AIs are discovered as part of the clinical workup for suspected adrenal disease (e.g. Cushing syndrome).
The differential diagnosis of AIs includes many primary, metastatic, benign, and malignant entities, most of which are not discussed at length here.
Adrenal cortical adenoma is a common benign tumor arising from the cortex of the adrenal gland. According to urology doctors, it commonly occurs in adults, but it can be found in persons of any age. Adrenal cortical adenomas are not considered to have the potential for malignant transformation.
Because adrenal metastases may be found in as many as 25% of patients with known primary lesions, radiologists frequently face the task of determining whether an adrenal mass is benign or malignant. The question can directly affect the clinical management of the case. For instance, the workup for an otherwise resectable lung cancer may reveal the presence of an adrenal mass and suggest the possibility of metastatic disease.
Causes
As per urologists, there are a number of causes. Some causes can make your adrenal glands produce too much of a hormone. This type of tumor is called a hormonally active or functional tumor. Hormonally active causes include:
- Cushing syndrome or subclinical hypercortisolism: conditions caused by too much cortisol
- Hyperaldosteronism: too much aldosterone
- A pheochromocytoma: a rare tumor in the adrenal glands that leads to too much epinephrine and norepinephrine
- Congenital adrenal hyperplasia: an inherited condition in which the adrenal glands make too little cortisol and aldosterone, and too much androgen
- Cancer of the adrenal gland with too much cortisol, adrenal androgens, and/or aldosterone
Other types of causes do not result in excess hormone production. This type of tumor is called a non-functional tumor. Causes include:
- An adenoma (a non-cancerous tumor in the adrenal glands)
- Cancer of the adrenal gland or spread of cancer from elsewhere in the body
- Cysts in or on the adrenal glands
- Other less common conditions, such as tumors filled with fat and blood cells
Symptoms
Even when discovered incidentally, adrenal tumors may cause symptoms. Symptoms vary depending on whether the tumor is non-functional or functional, and which, if any, hormones are produced in excess.
Symptoms of too much cortisol can include:
- Weight loss or weight gain (especially around the face and abdomen)
- Purplish skin stretch marks or skin that’s easily bruised
- Acne
- Muscle weakness
- Depression, anxiety, fatigue, and sleep disturbances
- In women, excess facial and body hair and/or irregular periods
High levels of cortisol can also cause high blood pressure, high blood sugar, and low bone density (when the tissue inside your bones starts to thin).
Symptoms of too much norepinephrine or epinephrine can include:
- Fast or irregular heartbeat
- Sweating
- Severe headaches
- Shakiness
- Pale face
- High blood pressure.
High levels of aldosterone can cause high blood pressure, which can be life-threatening if not treated, and sometimes muscle weakness.
Evaluation
Your urology doctor will evaluate your tumor to identify its cause and hormone production. This may include:
- Your medical history
- A review of your symptoms
- A physical exam: a check of your blood pressure, pulse rate, body weight, and other signs
- Blood and/or urine tests to check hormone levels and to rule out hormone excess
- Results of genetic tests (rarely)
Your doctor also will need to know your family history of adrenal tumors, other kinds of tumors, syndromes that come with tumors, high blood pressure, or Cushing syndrome.
Treatment
Nonsurgical treatment
Conditions that do not warrant surgery include bilateral adrenal diseases such as corticotropin-dependent Cushing disease or bilateral hyperaldosteronism. Nonfunctional (hormonally silent) adrenal cortical adenomas are not premalignant, and surgical excision is not indicated.
Surgical treatment
The treatment for a hormonally active adrenal tumor is surgery. The treatment for a malignancy depends on the cell type, spread, and location of the primary tumor.
No randomized trials have compared laparotomy versus laparoscopic adrenalectomy; however, abdominal laparotomy is preferred for bilateral disease, large masses (>10 cm), possible malignant disease, and pheochromocytoma. Fiberoptic laparoscopy is used for visualization, biopsy, and removal. A transthoracic approach is faster than fiberoptic laparoscopy but has a longer postoperative recovery period.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment
You must be logged in to post a comment.